Patients ask us on a daily basis to explain some of the terms they hear when going for a sleep study or read when they receive their sleep study results. We thought it would be helpful to compile a list of some of most commonly used terms.
Actigraph: A biomedical instrument for the measurement of body movement.
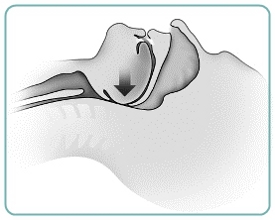
Apnea: Cessation of airflow at the nostrils and mouth lasting at least ten seconds. There are three types of apnea- obstructive, central, and mixed. Obstructive apnea is secondary to upper airway obstruction; central apnea is associated with a cessation of all respiratory effort; and mixed apnea has both central and obstructive components.
Apnea-hypopnea Index (AHI): The number of apneic episodes (obstructive, central, and mixed) plus hypopneas per hour of sleep as determined by all-night polysomnography.
Autotitration Device: A device that increases and decreases pressure in response to specific events, such as snore, flow limitation, apneas, and leak.
Bi-level Device: A device that provides two levels of positive pressure, one for inspiration (breathing in) and one for expiration (breathing out). Beneficial for some CPAP patients who are unable to tolerate high fixed pressures and for patients who present with hypoventilation.
Body Mass Index (BMI): Evaluates weight independent of height and may be correlated with mortality and other health-related factors. It is not a direct measure of body fatness and varies with body composition in relation to gender, age, and ethnicity. BMI= weight divided by height squared.
Central Sleep Apnea (CSA): Respiratory event that is characterized by no air flow for at least ten seconds during which no respiratory effort is evident.
Continuous Positive Airway Pressure (CPAP): A device that delivers continuous positive pressure to a patient's airway through an interface. The positive pressure acts as an air splint to keep the upper airway patent during sleep.
Electroencephalogram (EEG): A recording of the electrical activity of the brain by means of electrodes placed on the surface of the head. Together with EMG and EOG, EEG is one of the three basic variables used to score sleep stages and arousals.
Excessive Daytime Sleepiness (EDS): Subjective report of difficulty in maintaining the alert awake state, usually accompanied by a rapid entrance into sleep when the individual is sedentary; daytime tiredness or fatigue.
Hypersomnia: Excessively deep or prolonged major sleep period. May be associated with difficulty in awakening or sleep drunkenness.
Hypopnea: An episode of shallow breathing (airflow reduced by at least 50%) during sleep lasting ten seconds or longer, usually associated with an arousal or an oxygen desaturation.
Mixed Apnea: Respiratory event characterized by no air flow for at least ten seconds with both a central and obstructive component. The central component precedes the obstructive component.
Multiple Sleep Latency Test (MSLT): A series of measurements of the interval from "lights out" to sleep onset that is utilized in the assessment of excessive sleepiness. Subjects are allowed a fixed number of opportunities to fall asleep during their customary awake period. Excessive sleepiness is characterized by short sleep latencies. Long latencies are helpful in distinguishing physical tiredness or fatigue from true sleepiness.
Obstructive Sleep Apnea (OSA): Respiratory event characterized by no air flow for at least ten seconds with continuous respiratory effort.
Periodic Leg Movement (PLM): A rapid, partial flexion of the foot at the ankle, extension of the big toe, and a partial flexion of the knee and hip that occurs during sleep. The movements occur with a periodicity of 20-60 seconds in a stereotypical pattern lasting 0.5-5.0 seconds in duration and are a characteristic feature of the periodic limb movement disorder.
Polysomnogram (PSG): The continuous and simultaneous recording of physiological variables during sleep (i.e. EEG, EOG, EMG, EKG, airflow, respiratory movements, lower limb movements, and other electrophysiological variables).
Respiratory Disturbance Index (RDI): The number of respiratory events (apneas, hypopneas, and RERAS) per hour of total sleep time which cause an arousal or an oxygen desaturation as determined by all-night polysomnography.
Sleep-disordered Breathing (SDB): Describes a number of breathing disorders which occur during sleep, such as OSA, CSA, Cheyne-Stokes respiration, nocturnal hypoventilation.
Upper Airway Resistance Syndrome (UARS): Presence of repetitive arousals following periods of increased respiratory effort; are undetected by thermal sensors (i.e. thermistors or thermocouples) but can be identified by a nasal pressure transducer signal.
 Source: Glossary of Terms Used in Sleep Disorders Medicine, Resmed.
Source: Glossary of Terms Used in Sleep Disorders Medicine, Resmed.

 If you think you or someone you know may suffer from obstructive sleep apnea (OSA) or another sleep breathing disorder, there are several simple tests you can take. Be sure to always discuss your concerns with your health care provider.
If you think you or someone you know may suffer from obstructive sleep apnea (OSA) or another sleep breathing disorder, there are several simple tests you can take. Be sure to always discuss your concerns with your health care provider.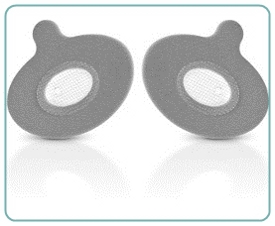 Approved by the Food and Drug Administration in 2008, Provent has spread mostly by word of mouth. But it has caught on fast. Its manufacturer, Ventus Medical, says it has shipped one million of the devices in the past 12 months, up from a half million total in the two years prior. Doctors say it has given them a new weapon in the battle against sleep apnea, and many patients who struggled with CPAP call it a godsend.
Approved by the Food and Drug Administration in 2008, Provent has spread mostly by word of mouth. But it has caught on fast. Its manufacturer, Ventus Medical, says it has shipped one million of the devices in the past 12 months, up from a half million total in the two years prior. Doctors say it has given them a new weapon in the battle against sleep apnea, and many patients who struggled with CPAP call it a godsend. According to DME MAC A, the Medicare Administrative Contractor for Durable Medical Equipment, more than two-thirds of all claims denied in their latest audit were denied because of issues with face-to-face clinical evaluation documentation.
According to DME MAC A, the Medicare Administrative Contractor for Durable Medical Equipment, more than two-thirds of all claims denied in their latest audit were denied because of issues with face-to-face clinical evaluation documentation.